Chordoma
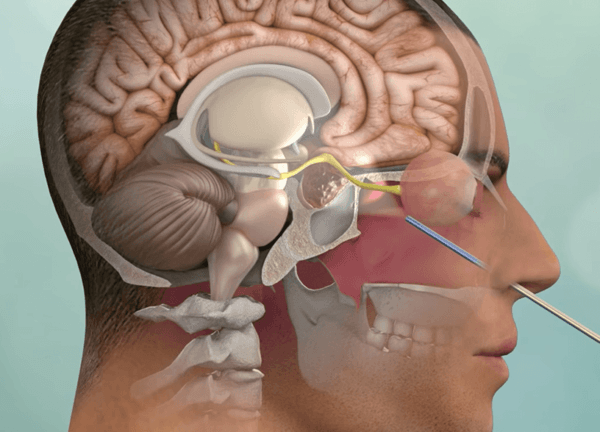
Endoscopic endonasal surgery is the preferred initial treatment for most Clival Chordomas
Clival chordomas are locally invasive tumors that arise in the base of the skull.
Clival chordomas are ideally treated with maximal safe surgical removal followed by focused radiotherapy. Fortunately, the majority of clival chordomas can be removed via the nose using an endoscopic endonasal approach. Occasionally, these tumors require multiple keyhole operations including the retrosigmoid and eyebrow craniotomy approaches.
At the Pacific Brain Tumor Center (BTC), we have one of the world’s largest experiences with endoscopic endonasal surgery for clival chordomas and a highly experienced surgical team. By incorporating cutting edge technology and instrumentation with proven surgical experience, we make chordoma surgery safer, less invasive and more effective. Given that many chordomas can be resistant to both surgery and radiosurgery, tumor genomic profiling is being increasingly used to find alternative targeted therapies.
Meet our multidisciplinary team
Learn more about our clinical trials
Read our chordoma-related publications
Overview
Chordomas are locally invasive slow growing malignant tumors that arise from the remnant of the primitive notochord.
They occur most commonly in the skull base (clivus) and lower spine; approximately 40% of chordomas and chondrosarcomas arise in the clivus (directly below the sella turcica and pituitary gland).
Chordomas can behave aggressively and are often extensively invasive into surrounding skull base structures. A small subset of patients (~10%) may develop metastases to distant sites beyond their site of origin.
Symptoms
The most common presenting symptom of a clival chordoma is double vision. Less common symptoms may include visual loss, hearing loss, difficulty swallowing, facial numbness, incoordination and motor weakness and nasal congestion.
Diagnosis
These skull base tumors are best diagnosed by MRI and CT scans which will clearly show the extent of tumor and bony destruction. Focused MRIs of the pituitary region, sinuses, temporal bones or internal auditory canals may be indicated to obtain better anatomical detail of a chordoma. Other tests may also be needed prior to surgery such as angiography (typically now performed as a CT angiogram or an MR angiogram), visual field tests, an audiogram or hormonal tests.
Treatment
Initial treatment for a clival chordoma is with surgical removal or debulking. Given their midline location, most clival chordomas and chondrosarcomas are best removed via an endoscopic endonasal approach. However, some extensive and/or laterally placed chordomas may require different skull base surgical approaches. Because chordomas typically invade the bone and dura of the skull base as well as cavernous sinus area, complete surgical resection is often not possible and continued growth of residual tumor is common. Extensive surgery can certainly improve long term survival but over aggressive tumor removal can be associated with significant neurological complications.
Most chordomas are treated after maximal surgical debulking with Stereotactic Radiotherapy (SRT), stereotactic radiosurgery (SRS) or proton beam radiation.
Additionally, while traditional chemotherapy has been relatively ineffective for chordomas, some new targeted agents are now available and showing promise in treating chordomas. At Pacific Brain Tumor Center, by using comprehensive tumor histological subtyping and genomic sequencing, we are able to provide a personalized therapeutic approach for each patient. Our Director of Neuro-Oncology, Dr. Santosh Kesari can facilitate clinical trial participation with novel medical therapies.
 Pituitary Gland & Pituitary Tumors Overview
Pituitary Gland & Pituitary Tumors Overview
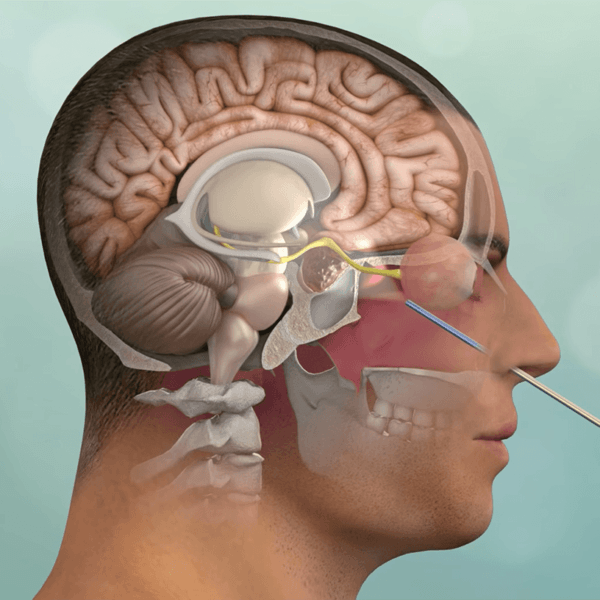 Endoscopic Endonasal Surgery Animation
Endoscopic Endonasal Surgery Animation
 Andrea’s Story – Clival Chordoma
Experience an actual account of Clival Chordoma.
Andrea’s Story – Clival Chordoma
Experience an actual account of Clival Chordoma.
Pituitary Gland & Pituitary Tumors Overview
Endoscopic Endonasal Surgery Animation